The AOSR uses cookies on its site to make your browsing experience better. By clicking OK, you agree to our terms of use. To find out more, visit our cookie policy.

| Chief complaint | This was a 69 years old man with left inguinal hernia claimed to be irreducible the night before admission. He self reduced the hernia upon admission but still complained of left lower abdominal pain and had repeated vomiting. Vitals were otherwise stable. |
|---|---|
| Age | 69yrs |
| Sex | Male |
| Modality | CT |
| System | Abdomen,Gastrointestinal |

Kwong Wah Hospital
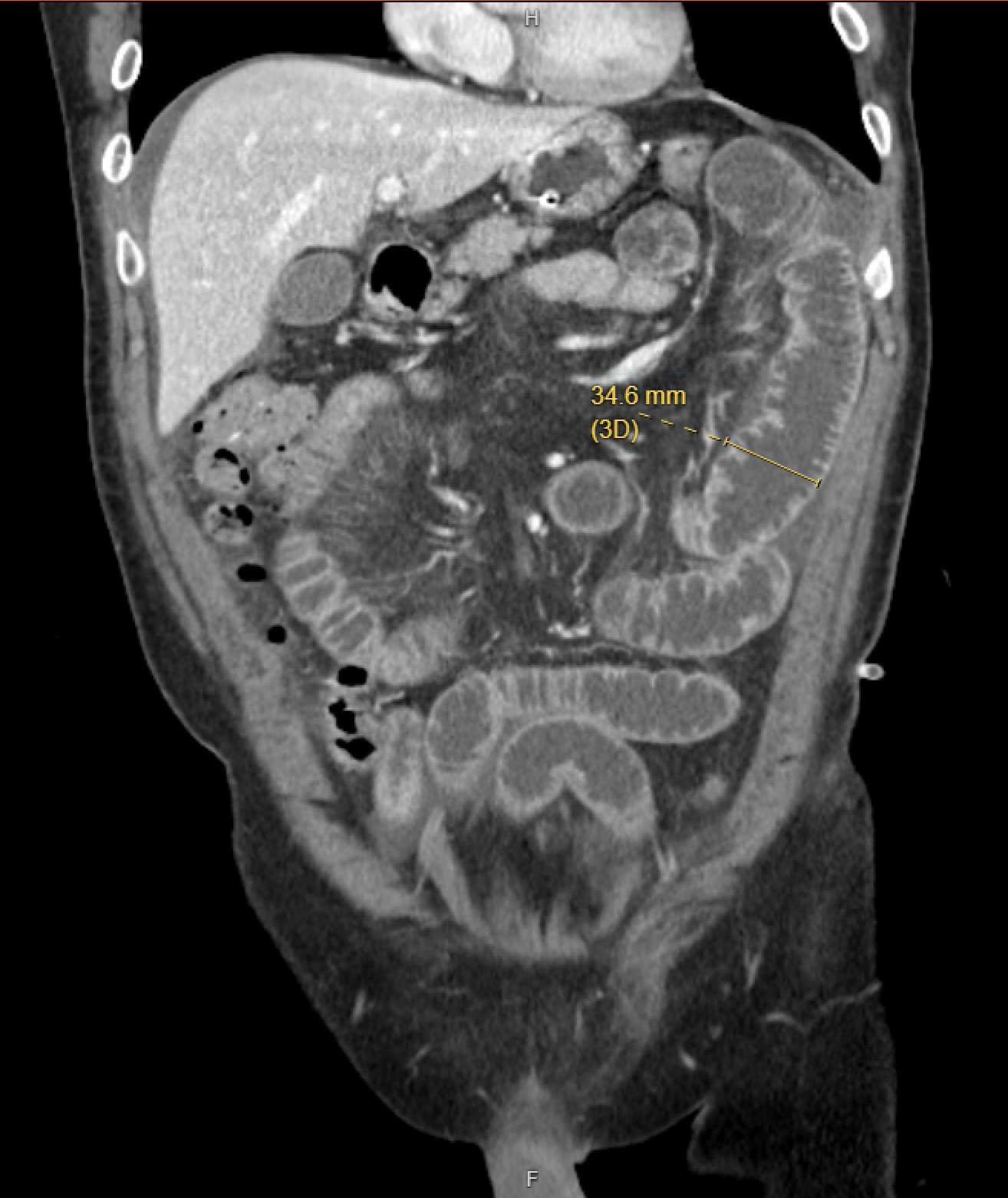
Reduction en-masse of left inguinal hernia with small bowel obstruction (SBO)
CT Findings: There are dilated small bowel loops involving the jejunum and proximal ileum. At left lower abdomen there is abrupt transition point at ileum with rest of ileal segment distal to transition point being non dilated suggesting mechanical small bowel obstruction. Large bowel is collapsed.
This transition point is closely related to left inguinal hernia, with hernia sac migrated into properitoneal space over left lower abdomen, associated with increased fat stranding,focal bowel mural thickening and adjacent fluid which could suggest incarceration or strangulation. A fibrous constriction band is also noted around the neck of the migrated hernia sac. Under such clinical context of recently reduced inguinal hernia, findings are suggestive of reduction en masse of left inguinal hernia, complicated with SBIO (Small bowel intestinal obstruction).
Clinical Progress:
Emergent operation was performed uneventfully on the day of CT scan, confirming the findings and diagnosis of reduction en-masse. Patient was discharged on day 10 after operation.
Clinical Significance:
"Reduction en masse of inguinal hernia" refers to a rare situation in which the hernial sac moves into the properitoneal space, leading to bowel incarceration. This condition involves the reduction of the hernial sac and its contents (mainly the bowels), resulting in a closed-loop obstruction.
The term is significant because urgent surgical treatment is crucial due to the potential complications associated with delayed intervention. Patients with this condition often present with a tender mass either high in the inguinal canal or in the lower abdomen on the side of reduction. A history of challenging reductions, with the last reduction being the most difficult, is common in these cases.
CT scan typically shows a fibrous constriction band at the neck of the hernial sac in the properitoneal space above the inguinal region. Prompt surgical intervention is necessary to prevent adverse outcomes, especially in cases where there is a delay from symptom onset to surgery.
Reference:
1. Ravikumar H, Babu S, Govindrajan M, Kalyanpur A. Reduction en-masse of inguinal hernia with strangulated obstruction. Biomed Imaging Interv J. 2009 Oct;5(4):e14
2. Akihiro Hoshino, Yasuyuki Kawachi, Susumu Takamatsu, Hiroto Nagano, Syunro Ohtsukasa, Syunsuke Kato, Hiroshi Maruyama, Reduction en masse can be treated using pure laparoscopic transabdominal preperitoneal hernioplasty following early CT diagnosis: report of a case, Journal of Surgical Case Reports, Volume 2015, Issue 5, May 2015, rjv055