The AOSR uses cookies on its site to make your browsing experience better. By clicking OK, you agree to our terms of use. To find out more, visit our cookie policy.

| Chief complaint | A 51 year old female presented with impaired right lower limb hemianaesthesia for temperature sensation since 1 year. Previously her complaints were affecting right lower limb up to the level of right knee but now the sensation abnormality had progressed up to right lower back with onset of mild right lower limb pain. Pin prick and tactile sensation were intact. She did not have any history of trauma or major illness. MRI thoraco-lumbar spine was performed and later CT myelography was also performed. |
|---|---|
| Age | 51 yrs |
| Sex | Female |
| Modality | CT/MRI |
| System | Musculoskeletal,Neurology |

Gujarat Imagining Centre
Gujarat Imagining Centre
Gujarat Imagining Centre
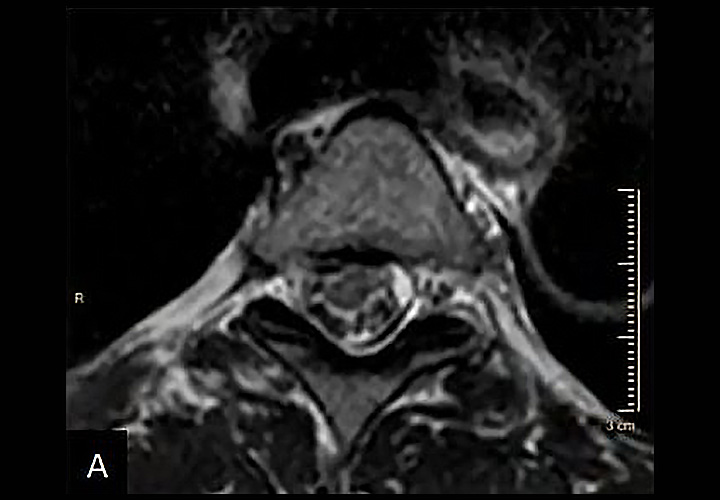
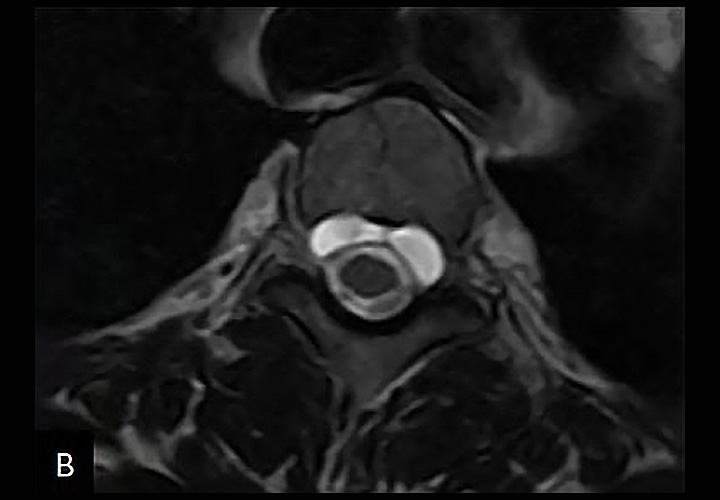
MRI findings (image A, B and C):
Focal distortion of the thoracic spinal cord is seen at T3 to T4 levels, appearing anteriorly displaced with resultant mild widening of dorsal CSF space giving 'Scalpel sign'. The thoracic cord at T3-T4 level is seen protruding through the dural sac at left antero-lateral aspect (at level of anterior funiculus) at T3-T4 level, suggests ventral cord herniation. No evident adjacent cord oedema is noted at the level of ventral cord herniation. It is associated with anterior intraspinal extradural CSF intensity loculated collection in cervico-thoracic region, most marked at T2 level. Disc osteophyte complex at T3-T4 level causing indentation over ventral aspect of dural theca.
CT myelography findings (image D):
Posterior osteophyte is seen at T3-T4 level Indenting dural theca. Intrathecal contrast is seen circumferentially opacifying the CSF space surrounding the cervico-thoracic cord. Thoracic spinal cord is seen anteriorly displaced and focally distorted at T3-T4 level with resultant widening of dorsal CSF space. Axial CT myelography images show focal ventral herniation of thoracic spinal cord at left anterior paramedian aspect, through the dural theca at T3-T4 level, just inferior to the above-mentioned posterior osteophyte at T3-T4 level. On delayed CT myelography images, contrast opacification of anterior epidural space extending from C6-C7 to T7- T8 level, most marked at T2 level suggest dural leak of contrast.